
We explain that the connection between psychology and neuroscience is remarkable in NeuroQuotient®. Although it is little explicit on the web. The relationship exists since the design of the model. NeuroQuotient was born from the answer to the question: What are the brain systems involved in the most frequent psychological disorders? We will see a graphic example about depression.
Professional people of psychology tell us that they appreciate a great potential to apply NeuroQuotient® in psychology. However, they do not see it reflected on the web.
They make us notice that we focus a lot on coaching and leadership, forgetting the connection between psychology and neuroscience that they see that NeuroQuotient® brings.
We can do nothing but accept that they are right. In both comments. Actually, there are Certified psychologists in the neuro tool who are using it with remarkable success with their clients. And because the connection between psychology and neuroscience provided by NeuroQuotient® is very powerful (and simple) and it is not explicit on the web.
We forget to reflect the application of neuroscience in psychology through our tool, because for us it is very obvious. This is because of the origin of the model (as we will see) and the results we are obtaining.
Also, we have not wanted to focus on the relationship between psychology and neuroscience for a couple of other reasons.
Too many times, going to the psychologist sounds like a ‘disorder’, so we prefer to talk about self-leadership development.
The first reason is simply marketing regarding coaching. For many patients and clients, from professional settings, it is much more acceptable to say that they work with a coach than with a psychologist, right?
The other reason is related to the language we use in NeuroQuotient. It is observable that when we talk about coaching and leadership, we never refer to leadership development. We always talk about self-leadership. One cannot be prepared to lead others if one does not lead oneself.
To make clear the connection between psychology and neuroscience provided by NeuroQuotient, we will start a series on neuroscience and psychology. In the current article, we will give a visual example of a disorder that we treat in another post: depression. In addition, depression shows one of the low levels of self-leadership.
But, before, it is important that we comment on the connection between psychology and neuroscience through NeuroQuotient. We are going to explain, neither more nor less than the strategy we follow for the design of the model.
The key to structuring the NeuroQuotient model was to identify brain systems and neuro behaviors associated with psychological disorders.
To design NeuroQuotient, we start from a question: What are the brain systems that are involved in the most common psychological disorders? Disorders such as anxiety, depression, attention deficit, etc. From there, we believe that it is not necessary to say much more:
The connection between psychology and neuroscience is at the origin of our model and tool. It is one of the few psychobiological models that explain behavior from the biology and the brain.
The connection between psychology and neuroscience that we provide is not only a lever to take advantage of neuroscience in psychology. It can also be useful to take advantage of it in psychiatry. Psychiatrists, doctors, have in their hands a powerful weapon: drugs. NeuroQuotient can be an opportunity for some psychiatrists, to review how to use the pharmaceutical resource in a more effective way.
An example. The graphic visualization of depression healing.
The reason for this post on psychology and neuroscience is not to explain the structure of the neuro-tool. You can see this in one of our free introductory workshops. Nor will we go deep into what we understand are the neurological foundations of depression.
Regarding the second point (neuro fundamentals) we can comment that in the certification as Practitioners, coachs, psychologists, etc. understand, for example, that increasing serotonin is not always the best way to treat depression. This neurotransmitter, so fashionable, we believe it is not a panacea. It is related to behavioral inhibition and it is difficult to find greater inhibition than in depression. In addition, the genetic profiles with a greater tendency towards this disorder have more serotonin available at their synaptic clefts.
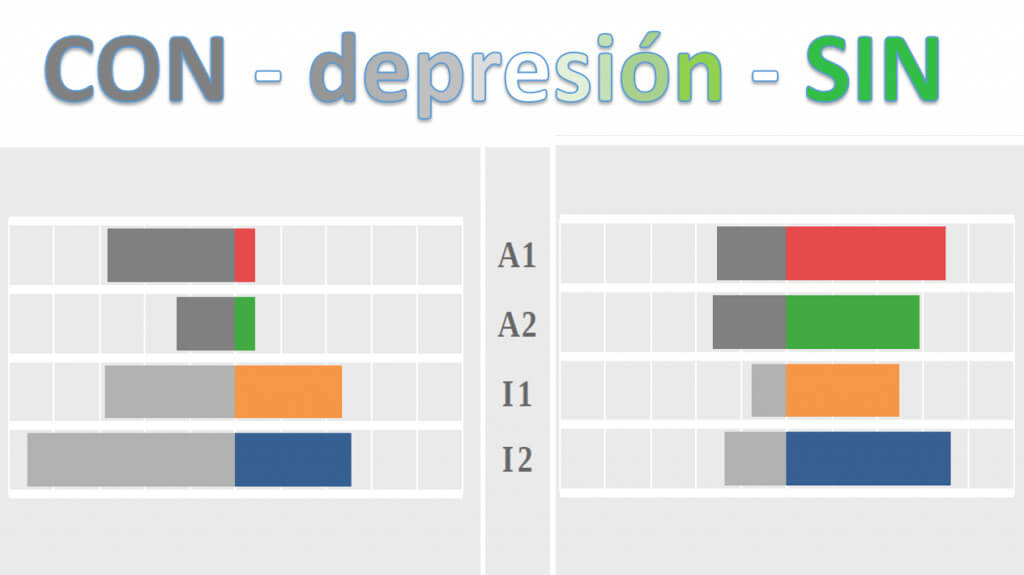
As for the structure of NeuroQuotient, just a couple of notes to understand the graph that follows. It is a very visual tool that measures neuro behaviors. Neuro behaviors are brain processes in doing, thinking and feeling with a neuronal substrate. We call efficiencies those neuro behaviors that give us good emotional results and we paint them in color. We call limitations those who do not help us with our satisfaction and draw them in grey.
That said, the following graphs, Fig 1, correspond to a real case of a person with depression (left side) and the same person without depression (right side). The time elapsed between the first and second graph was approximately 6 months. Both pictures, as you can imagine, result from answering a questionnaire.
At first glance it can be seen that there is much more color and less gray in the graphic on the right (without depression). It is indicating a higher level of satisfaction of the person. The efficiencies are higher and the limitations lower. And it is not a case of bipolar disorder, we know that depression is consistently overcome a few years later.
Specifically, the greatest progress is seen in the reduction of the I2 limitation, directly related to depression.
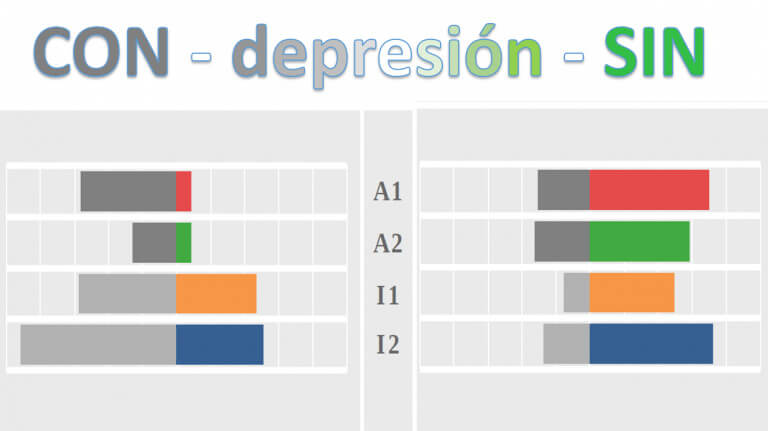
Attention! Neither personality nor diagnosis. Only to guide and visualize progress.
We want to believe that the connection between psychology and neuroscience through NeuroQuotient is more evident after this example. But allow us to remark three important final notes:
One. The example makes it clear that we are not facing a personality tool. The person is the same in the chart on the left and the one on the right. In six months, the personality of an adult is not able to change.
Two. We do not aim, and do not want, that it serves for the diagnosis. But it is very useful to assess the ‘moment’ of the person who asks us for support and to better guide them according to their needs.
Three. The client (patient, coachee, etc.) can visualize their progress at the end of a process. This is very powerful and has a great enhancing effect on the client.